Alteration of tissues in acute inflammation:
Alteration of tissues in acute inflammation are described in two phases: Vascular events and cellular events.
Vascular events:
A. Arteriodilation:
Immediately after tissue injury, there is transient constriction of blood vessels due to neurogenic effects. This is soon followed by vasodilatation. Arteriodilation is carried out by the effects of histamine and other chemical mediators like prostaglandin, leukotrienes.
Injury of tissue —–>Mast cells release histamine and other mediators———->
Histamine acts on smooth muscle of arterioles ———–> Relaxation of smooth muscles——-> Blood flow increases due to relaxation of muscle
B. Changes in rate of flow:
I. Increased Vascular Permeability:
The endothelial wall of capillaries and venules forms a semi-permeable barrier that allows free movement of water and small molecules and is only slightly permeable to plasma proteins.
After inflammation proceeds these membrane permeability increases due to following reasons:
Mechanism of increased vascular permeability:
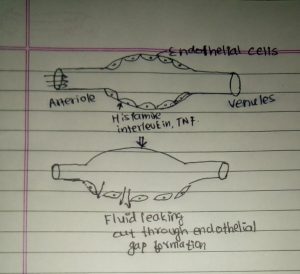
a. Formation of endothelial gaps:
Normally endothelial cell in arterioles have tight junction. But when tissue is injured, chemical mediators released by mast cell acts on endothelial cell. Histamine, bradykinin, and leukotrienes (LT4) acts on endothelial cell and causes contraction of endothelial cell. This causes formation of endothelial gaps.
Similarly, as time passes, there is further release of cytokines. Cytokines act on endothelial cells of arterioles and causes retraction of endothelial cells. This leads to formation of gaps in endothelial cells.
b. Direct endothelial injury:
- In this case, there is disruption of endothelial lining due to which endothelial gaps are produced.
- It is mainly observed in severe injuries like burns or infections.
- This reaction is also called immediate sustained response.
c. Delayed prolonged increased permeability:
- This usually occurs in direct endothelial injury. There may be delayed prolonged leakage.
- It usually starts after 2-12 hours and remains for several days.
- It is due to delayed production of cytokines.
- Mild to moderate thermal injury, bacterial toxins, UV-radiation, X-rays may produce this condition.
d. Leukocyte-mediated endothelial injury:
- It is primarily seen in pulmonary microcirculation and glomerular microcirculation.
- Endothelial cells in these areas hold neutrophil for longer time. So, they are more prone to this type of injury.
- Toxic metabolites such as reactive oxygen species and proteolytic enzymes liberated by leukocytes causes endothelial injury and increases vascular permeability.
e. Increased transcytosis:
- It occurs through intercellular vesicular pathway. There is formation of vesicles on vascular side and transfer to basal side of endothelial space.
- Channels forms through fusion of uncoated vesicles through which transcytosis occurs.
f. Excessive leakage of fluid from newly formed vessels:
- Certain growth factors leads to formation of new blood vessels. These new vessels donot have much endothelial junction or there is not so tight endothelial junction. They get leak until they gets matures.
II. Slowing of circulation:
But increased blood flow to site of injury is soon followed by slowing of circulation. This is termed as stasis. Slowing of circulation is due to increased vascular permeability. Increased vascular permeability causes increased in hydrostatic pressure in arterioles.
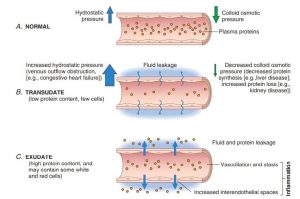
Normally, blood flow is in linear pattern. This is usually maintained by two pressure: hydrostatic pressure and osmotic colloidal pressure. Hydrostatic pressure in arterioles side is decreased and osmotic pressure is stable but in case of venules it is opposite. Thus, fluid leaking in small amount gets back into circulation from venules in normal cases.
But in case of increased vascular permeability, hydrostatic pressure is greatly increased, and osmotic pressure decreases. Due to this there is excessive leakage of fluid which cannot gets back into circulation and accumulates in interstitial space.
Due to exudation of plasma proteins, blood becomes more viscous and blood flow is decreased. This is essential for emigration of leukocyte, mainly neutrophil.
III. Stasis:
As soon as blood becomes more viscous, flow of blood decreases greatly and stasis is produced.
C.Changes in the Bloodstream:
- The main change consist of redistribution of cellular elements in bloodstream.
- In normal circulation, there is two distinct zones: central part contains cellular elements ( leukocytes and erythrocytes) which is called axial stream and external to axial stream there is plasmatic stream which is clear zone of plasma.
- The cellular elements are held in centre by centripetal force of flowing blood. As blood flow slows down, centripetal force of bloodstream is overcome by centrifugal force and leukocyte fall out of axial stream. This process is called margination.
- After leukocyte falls down, they tumble slowly along the endothelial surface and adhere transiently. This process is called rolling.
- Finally, leukocytes comes to rest at point where they adhere firmly. This process is called adhesion. In this process, endothelium is lined by white cells which is known as pavementing.
D. Exudation of Plasma:
- Due to increase vascular permeability, plasma fluid escapes out to extravascular space. This process is called exudation.
E. Emigration of leukocytes:
- It is the process by which leukocytes comes out of blood vessels into extravascular space.
F. Diapedesis of Erythrocytes:
- Following emigration of leukocytes, red cells are pushed out of vessel passively by intravascular pressure. This is called diapedesis.