Equine encephalitis:
Syn: Equine viral encephalomyelitis, Equine sleeping sickness
- It is a infectious viral disease affecting horses.
- It is characterized clinically by signs of deranged consciousness, molar irritation and paralysis.
Etiology:
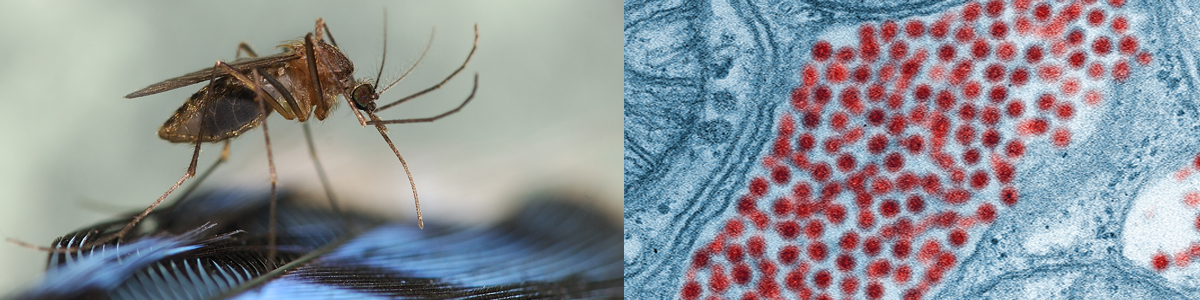
- α-virus of Togaviridae family
- virus have three strains; eastern, western, Venezuelan
- eastern strain is most virulent whereas western is less.
- Horses, Donkey, Mule, Monkey and Man are naturally affected.
Epidemiology:
- These viruses are endemic to North, Central or South America
- The North American variant is the most pathogenic and is found in eastern Canada, all US states east of the Mississippi River, Arkansas, Minnesota, South Dakota, Texas; and in the Caribbean islands. The South American variant, now called Madariaga virus (MADV), is less pathogenic and is confined to Central and South America.
- EEEV is perpetuated in a sylvatic cycle between avian hosts (passerine birds) and mosquitoes, with primary transmission in this cycle via Culiseta melanura.
- Snakes have been identified as a possible reservoir.
- Young horses are more susceptible. Disease mostly occurs in mid and late summer.
- Incubation period; 1-3 days in EEE, 2-4 days in WEE, and 1-6 days in VEE
Transmission:
- Disease is primarily transmitted through bite of insects, i.e. mosquitoes, ticks, bugs, mites and lice.
Pathogenesis:
- Virus gains entry through bite of mosquitoes
- After entry, they replicate at entry sites including dendritic cells
- Dendritic cells transport virus to regional LN
- It is followed by primary viremia
- Virus then invades extraneural fissures, multiplies leading secondary viremia.
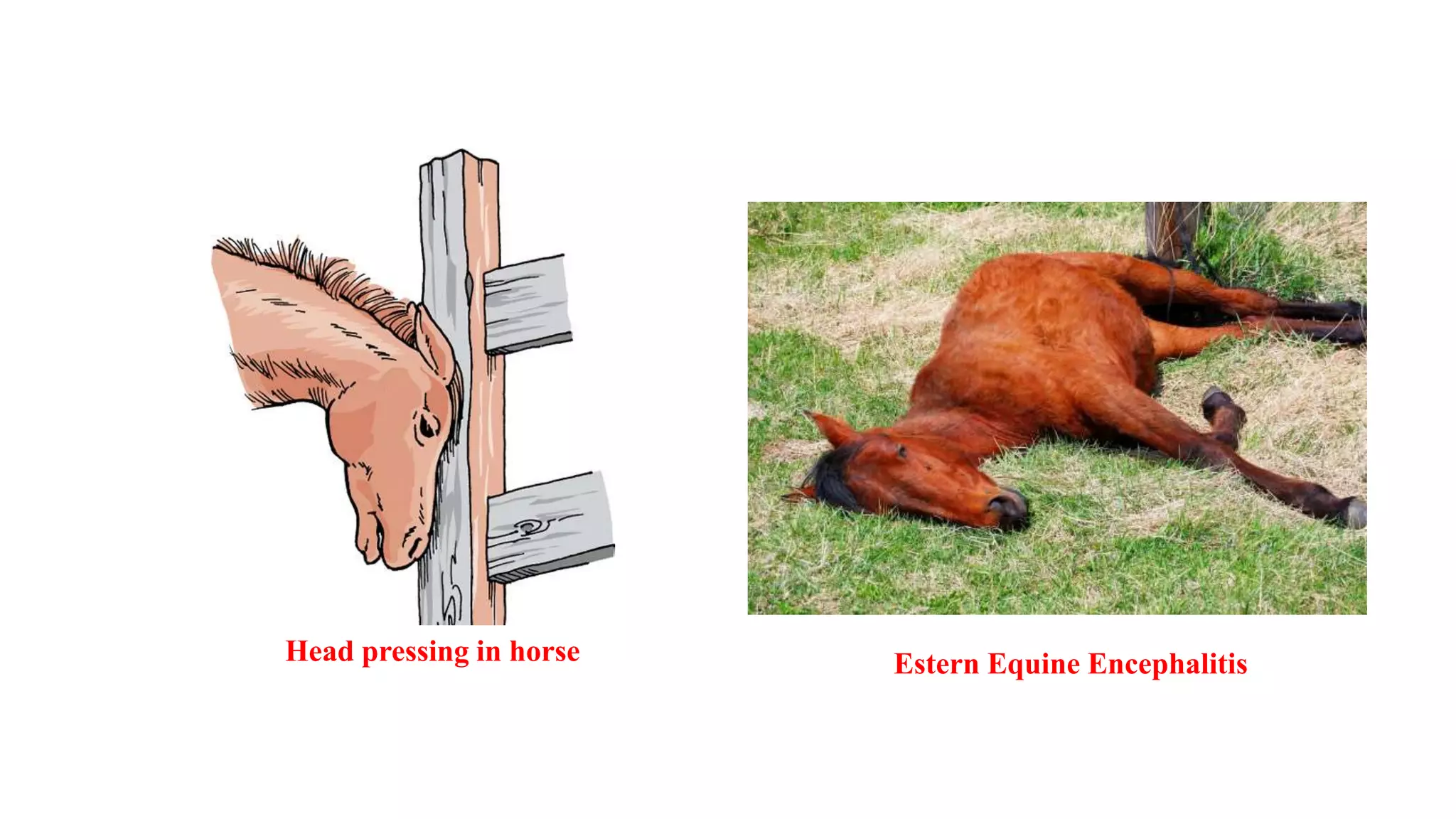
Clinical Signs:
- Initially fever with anorexia, depression
- Temperature increases upto 24-48 hours (106°F). Nervous signs occurs at peak of temperature rise.
- Abnormally wide stance, hanging head, dropping ears, flaccid lips
- Aimless walking, central blindness
- Inability to swallow, photophobia, circling, yawning, grinding of teeth
- Constant head pressing against a corner or stall or fence is typical presentation.
- Death occurs within 2-3 days after onset of clinical signs
Diagnosis:
- Isolation and identification of virus
- HI, CFT, VNT, ELISA
- PCR
Treatment and Control:
- There is no effective antiviral treatment available for disease. Supportive care is advised.
- To control pain; flunixin meglumine @1.1 mg/kg, b.wt. IV every 12 hours upto 5 days
- Phenobarbitone or Diazepam to control convulsion.
- Hyperimmune serum 500 ml, IV
- Neurobion; B12 injection 3000 mcg @ 1-2 mL, IM or SC
- Vaccination; Live attenuated vaccine used intradermally.